Things that Sting and other dangerous Marine Life.
Note:
It is not possible to identify all types of potentially harmful marine life and the chances or types of injury. Local medical personnel are an additional source of information and should be consulted prior to diving in unfamiliar waters. A good working knowledge of the marine environment will prevent lost time or severe injury. This article deals with marine life in the Caribbean- Atlantic Oceans.
All Photos by Barb Crites, St. John, USVI.
Information condensed from the U.S Navy Diving Manual. Volume 5
Scroll down or Go To:
URCHINS -
CORAL -
BRISTLE WORMS -
SPONGES -
JELLYFISH -
VENOMOUS FISH -
BARRACUDA -
PUFFERFISH-
STINGRAYS -
MORAY EELS -
SHARKS -
CIGUATERA and SCOMBROID FISH POISONINGS

Sea Urchins
There are various species of sea urchins with widespread distribution. Each species has a radial shape and long spines. Spines will break off and remain in the wound causing localizes pain for a brief period. The embedded spines give off a deep purple dye. The spine will dissolve in a few days. Should puncture wounds be very numerous, be prepared to treat for shock. Even the short-spined sea urchin can produce a painful puncture wound if contacted even gently.
Prevention
Always be aware of your surroundings, look around before free diving, taking photo or other activities in close quarters and in shallow water. Do not step without looking. Spines can penetrate wet suits, booties, and even tennis shoes. If it’s not sand, don’t stand.

First Aid and Treatment
1. If possible, remove large spine fragments gently.
Small fragments may be absorbed by the body.
2. Bathe the wound in vinegar or isopropyl alcohol. Soaking the injured extremity
in hot water up to 122ºF (50ºC) may help. Caution should be used to prevent
scalding the skin which can easily occur after a brief period in water above
122ºF (50ºC).
3. Clean the wound of all foreign objects. Use an antibiotic ointment to prevent infection. Watch for possible secondary infections.
4. A tetanus shot may be advised.
5. Get professional medical attention for
multiple, deep wounds.
Rock Boring Urchin (red and black)
Long Spine Urchin
Reef Urchin
Slate Pencil Urchin
West Indian Sea Egg Urchin
Variegated Urchin

Coral
Coral is extremely sharp and the most delicate coral is often the most dangerous because of their razor-sharp edges. Coral cuts, while usually fairly superficial, can take a long time to heal. The smallest cut, if left untreated, can become ulcerous. Watch for secondary infections indicated by the presence of a red and tender area surrounding the cut.
Prevention
Extreme care should be used when swimming/diving near coral. Often coral is located in a reef formation in areas of wave surges, surface current, and bottom current. Be prepared. Strong waves can tumble a person over a coral reef causing damage to the reef and possible sever injury to the person. Coral should not be handled with bare hands. Never stand where coral is present. In any kind of surge, calculate a safe distance away from a coral reef, and then double it.

First Aid and Treatment-Coral cuts and abrasions
1. Stop any bleeding that may occur.
2. Clean promptly with hydrogen peroxide or over-the-counter iodine solution and remove dead, contaminated, or adherent tissue and/or foreign material.
3. Bandage the wound.
4. A tetanus shot may be recommended.
5. Topical antibiotic ointment has been proven very effective in preventing secondary infection.
Stinging coral wounds (Fire Corals)
may require symptomatic management such as topical steroid therapy, systemic antihistamines, and analgesics. In severe cases, bed rest is required to elevate the extremity, wetto-dry dressings, and systemic antibiotics. Systemic steroids may be needed to manage the inflammatory reaction resulting from a combination of trauma and dermatitis.

Bristle Worms
Segmented Bristle Worms have long, segmented bodies with stinging bristle-like structures on each segment. These fiberglass-like spines easily become embedded in human flesh.
Prevention
Avoid touching or stepping on bristleworms. Do not reach under or into recesses.

First Aid and Treatment
1. Remove bristles with a very sticky tape such as adhesive tape or duct tape.
2. Topical application of vinegar will lessen pain.
3. To relieve symptoms use topical steroids, antihistamines, and analgesics.
4. Wound infection can occur but can be easily prevented by cleaning the skin using over the counter iodine and topical antibiotic ointment. Seek medical advice if infection worsens.

Sponges
Sponges are composed of minute multicellular animals with spicules of silica or calcium carbonate embedded in a fibrous skeleton. Exposure of skin to the chemical irritants on the surface of certain sponges or exposure to the minute sharp spicules can cause a painful skin condition called dermatitis.
Prevention
Avoid contact with sponges and wear gloves when handling live sponges.

First Aid and Treatment
1. Adhesive or duct tape can effectively remove the sponge spicules.
2. Vinegar should be applied with saturated compresses as sponges may be secondarily inhabited by stinging hydroids.
3. Antihistamine lotion (diphenhydramine) and later a topical steroid (hydrocortisone), may be applied to reduce the early inflammatory reaction.
4. Antibiotic ointment is effective in reducing the chance of a secondary infection.

Jellyfish, Anemones and Hydroids
Jellyfish vary widely in size and color from blues, reds and browns to transparent. They swim suspended in the water, generally with a pulsating movement, or float on the surface. All have stinging tentacles that sting and trap prey. Jellyfish stings are the most common stinging injury. They inhabit the oceans worldwide. Anemones attach themselves to structures or bury their bodies in cracks and crevasse with only tentacles visible. Both jellyfish and anemone’s tentacles have organs in the tentacles called nematocysts. While most stings result only in painful local skin irritation, the Portuguese man-of-war is the most dangerous type, and deaths from Portuguese man-of-war stings have been reported.
Prevention
Never handle jellyfish. Specimens found on shore, or those that appear dead may still be able to sting. Even towels or clothing contaminated with the stinging nematocysts may cause stinging months later. Avoid Tentacles. Jellyfish tentacles can trail the body of the jellyfish up to 165 feet in length, (Portuguese man-of-war) but most common 10 feet horizontally or vertically in the water and are not easily seen. Avoid close proximity to jellyfish to avoid contacting their tentacles. Protecting yourself. Wear a wet suit, body shells, or other protective clothing when in waters where jellyfish are abundant. Petroleum jelly applied to exposed skin (e.g., around the mouth) helps to prevent stinging.
 Upside down Jelly
Upside down Jelly Highly toxic stinging cells. Turtle grass anemone
Highly toxic stinging cells. Turtle grass anemoneFirst Aid and Treatment.
Without rubbing, gently remove any remaining tentacles using a towel or clothing. For preventing any further discharge of the stinging nematocysts, USE vinegar.
DO NOT:
1. use alcohol or preparations containing alcohol. Alcohol plus seawater mixtures have all been demonstrated to cause a massive discharge of the nematocysts. In addition, these compounds may also
worsen the skin inflammatory reaction.
DO NOT
2. Use picric acid, human urine, and fresh water.
They have also been found to either
be ineffective or even to discharge
nematocysts. DO NOT:
3.Rub sand
or apply papain-containing meat tenderizer.
It is ineffective and may lead to further nematocysts discharge and should not be used.
It has been suggested that isopropyl (rubbing) alcohol may be effective. It should only be tried if vinegar is not available.
Symptomatic Treatment. Symptomatic treatment can include topical steroid therapy, anesthetic ointment (xylocaine, 2 percent) antihistamine lotion, systemic antihistamines or analgesics. Benzocaine topical anesthetic preparations should not be used as they may cause sensitization and later skin reactions. Anaphylaxis. Anaphylaxis (severe allergic reaction) may result from jellyfish stings.

Venomous Fish
There are two levels of venomous fish. Those that pose a lesser degree of serious injury and those that can cause serious reactions and possible death given the right circumstances. Those fish that pose the most danger are the Indo-Pacific Lionfish, an invasive species, Scorpionfishes, and Stonefish, which are not found here in the Caribbean. Occasionally stings can occur without knowing the species. Venomous fish are not known to be aggressive and stings may occur by accidentally stepping on one or encountering a dead fish on the beach. Spines remain venomous even after the fish is dead. All venom is thought to be generally affected by the application of heat (hot water) to the wound. Heat decomposes the toxin. Local symptoms of a venomous sting include severe pain (compared to what would be expected), numbness or hypersensitivity around the wound. The wound site may become swollen and tender, having a pale color and cyantonic discoloration in the center (due to not enough oxygen in the blood in surrounding tissue). Other expected symptoms include nausea, vomiting, sweating, mild fever, respiratory distress and collapse. The possibility of anaphylactic shock is a clear danger and should not be discounted.
Prevention
Venomous fish are generally well camouflaged bottom dwellers, or occupy holes or crevices Do not reach into holes recesses or crevasses. If it is not sand, don’t stand. Avoid fish washed up on shore unless you can positively identify.
Indo-Pacific Lionfish
Plumed Scorpionfish
Reef Scorpionfish
Spotted Scorpionfish
.jpg)
First Aid and Treatment-Moderate Toxins
1. Get victim out of water; watch for fainting and signs of shock.
2. Lay the victim down and reassure.
3. Wash wound with cold, salt water. Do not try to remove toxin by suction. Surgery may be
required to open up the puncture wound.
4. Soak wound in hot water for 30 to 90 minutes. The water should be as hot as the victim can tolerate but not hotter than 122ºF. If temperature is not calculable, immerse both limbs. The unaffected limb will ensure the water temperature is tolerable. This will prevent burns to the affected wound site. Use hot compresses if the wound is on the face. Adding epsom salts to the water does not help.
5. Take a muscle relaxer (diazepam, valium) to help reduce muscle spasm.
6. Do not use a tourniquet. Remove traces of spine and sheath since the sheath may continue to release venom.
7. Use an antiseptic or antibiotic ointment and sterile dressing. Try to restrict movement of the extremity by using splints or slings.
9. If first aid is not administered within a short time, consult a medical professional as to the proper treatment. A tetanus shot may be recommended
First Aid and Treatment-Highly Toxins
. In the case of a sting from highly toxic Zebrafish/Lionfish, Scorpionfish or Stonefish. Give the same first aid as that given for other venomous fish. Pain may persist for days rather than hours. Seek professional medical treatment if respiratory failure and cardiovascular collapse is suspected. An antivenin has been developed for Stonefish toxin but may have some beneficial effects against the scorpionfish and zebrafish/lionfish.
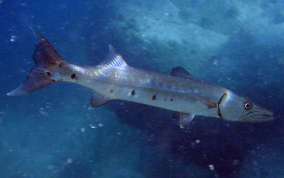
Barracuda
The barracuda is a long, thin fish with a long V-shaped jaw and large teeth. They have a forked tail and are generally green to bluish gray. Their back scales often glisten in a random sparkle and they usually have random, dark blotches on their sides.. The Great Barracuda of the Caribbean can grow up to six feet in length and is capable of striking with amazing speed and veracity. It is known to follow a swimmer or snorkeler out of curiosity, but seldom attacks. It is known to attack limbs dangling in the water on rare occasions. Barracuda bites are distinguishable from shark by the pattern. A barracuda leaves a V-shaped or straight wound, shark wounds have a curved outline. Attacks by barracuda are rarely life threatening.

Prevention
Barracuda are attracted by bright objects. Avoid shiny equipment and remove jewelry. Barracuda have been known to strike at fish being carried underwater (as in spearfishing). Avoid splashing or dangling limbs in waters that the Barracuda inhabit
First Aid and Treatment.
Follow the same as those used for shark bites although injuries most likely will be less severe than shark bites.

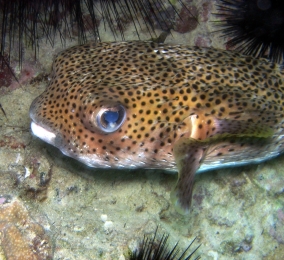
Balloonfish and Puffers
These fish have sharp spines and jaws that can break fingers. Their main defense, used as a last resort when cornered or molested is to overinflate their bodies with either air or water. This trick takes a toll on the fish and a new study shows that fish can become easy prey once they are deflated again.
Prevention
Protect yourself and the lives of these fish. Do not molest these generally shy and gentle creatures.
First Aid and Treatment
1. Stop any bleeding from Bites.
2. If possible, remove large spine
fragments gently. Clean the wound of all foreign objects.
3. Use an antibiotic ointment to prevent infection. Watch for possible secondary infections.
4. A tetanus shot may be advised.

Stingrays
The Southern stingray is the only stingray common to the north eastern Caribbean. It will burrow into sand with only eyes and tail exposed Approximately 1,800 stingray injuries are reported annually in the U.S. Most injuries occur when they are accidentally step on. The ray will lash its tail defensively and the spine, located on the tail near the base will puncture or lacerate the flesh. The wound will swell and pale with a blue rim. Secondary localized infections are common. The toxin may cause fainting, nausea, vomiting, sweating, respiratory difficulty, and cardiovascular collapse

Prevention
In shallow sandy or grass bottomed , shuffle rather than walk on the bottom. If possible, probe the surrounding area with a stick to alert the rays and encourage them to leave.
First Aid and Treatment.
Give the same first aid as that given for venomous fish. No antivenin is available.

Moray Eels
Moray Eels are inhabitants of reef environments, and are found in recesses and under rocks and coral. Some hunt during the day and others at night. The Green Moray can grow to a length of eight (8) feet while others are much smaller at thirteen (13) inches. Although eels look and behave much like snakes, they are not snakes. Morays are territorial and bites can occur when reaching into their space. Morays, once they bite are very difficult to dislodge. They have a second set of jaws in their throats called pharyngeal jaws, which also possess teeth. When feeding, morays launch these jaws forward into the mouth, where they grasp prey and transport it into the throat and digestive system. Moray eels are the only animal that uses pharyngeal jaws to actively capture and restrain prey. Larger morays are capable of seriously wounding humans. Most injuries are to hands and arms

Prevention
Never reach into holes or crevasses. Do not tease, feed or try to dislodge an eel from its hole.
First Aid and Treatment.
1. Stop the bleeding using direct pressure and raising the limb. Severe hand injuries should be evaluated for muscle, tendon and nerve damage. Surgical repairs may be necessary to prevent permanent loss of hand/limb function.
2. Certain eels have toxins in the oral mucus. Treatment for envenomation may be advised.
3. A tetanus shot may be warranted.
4. Antibiotics may be administered.
Chain Moray Eel
Chestnut Morey
Goldentail Moray Eel
Green Moray Eel
Purplemouth Moray Eel
Spotted Moray Eel

Sharks
Shark attacks on humans are
infrequent but possible. Only 30 of
the 460 shark species in the world,
have ever attacked humans and only a
handful are repeat offenders and are
also big enough to be considered
dangerous to people. According to
the International Shark Attack File
the 2014 yearly total of 72
unprovoked attacks was lower than
the 75 recorded in 2013 and
represents the lowest global total
since 68 in 2009.
Except for the
Bahamas, West End, Grand Bahamas'
Island, which is frequented by
sharks, notably Tigers Sharks,
Caribbean attacks are very rare. In
general shark attacks are
unpredictable. Injuries may result
not only from bites, but also by
coming in contact with the shark’s
skin. Shark skin is covered with
very sharp denticles, which are
reinforced with tooth-like centers.
Contact with it can lead to wide
abrasions and heavy bleeding.
Shark Pre-Attack Behavior.
A shark swimming with an exaggerated motion, its pectoral fins pointing down in contrast to the usual flared out position and swimming in circles of decreasing radius around its prey can be considered in ‘attack mode’. An attack may be also be recognized by other marked changes in behavior, unexpected acceleration or postures, or swim patterns. If you notice other marine life becoming agitated, that may forewarn the presence of a shark in the area. No one can outswim a shark. All sharks must be treated with extreme respect and caution especially when spearfishing or chum of any type is in the water.

First Aid and Treatment.
CALL FOR EMERGENCY MEDICAL HELP AS
SOON AS POSSIBLE
1. Bites often
result in a large amount of bleeding and
tissue loss. Take immediate action to
control bleeding with whatever available
for use as pressure bandages. Cover
wounds with layers of compressive
dressings easily made from shirts or
towels, then wrap tightly with gauze,
torn clothing, towels, or sheets. Use
direct pressure on elevated limb or
extreme compression on pressure points
will control all but the most serious
bleeding. The major pressure points are:
the radial artery pulse point for the
hand; above the elbow under the biceps
muscle (brachial artery) for the
forearm; and the groin area (femoral
artery) with deep finger-tip or
heel-of-the-hand pressure for bleeding
from the leg When bleeding cannot be
controlled by direct pressure and
elevation or pressure points, a
tourniquet or ligature may be needed to
save the victim’s life even though there
is the possibility of loss of the limb.
Tourniquets are applied only as a last resort and
with only enough pressure to control
bleeding. Do not remove the tourniquet.
The tourniquet should be removed only by
a physician in a hospital setting.
Loosening of a tourniquet may cause
further shock by releasing toxins into
the circulatory system from the injured
limb as well as continued blood loss.
2. Treat for shock. Lay the victim down
and elevate his feet. Keep him warm.
3. Transport the victim to a medical
facility as soon as possible. Reassure
the
victim.
4. Should a severed
limb be retrieved, wrap it in bandages,
moisten with saline,
store in a
plastic bag and chill, separating the
tissue from direct contact with ice.
Transport the
limb with the patient.

Fish Poisonings
Ciguatera Poisoning
Ciguatera poisoning is caused by eating the flesh of a fish that has eaten a toxin-producing microorganism, the dinoflagellate, Gambierdiscus toxicus. The poisoning is common in reef fish between latitudes 35ºN and 35ºS around tropical islands or tropical and semitropical shorelines in Southern Florida, the Caribbean, the West Indies, and the Pacific and Indian Oceans. Fish and marine animals affected include barracuda, red snapper, grouper, sea bass, amberjack, parrot fish, and the moray eel. Incidence is unpredictable and dependent on environmental changes that affect the level of dinoflagellates. The toxin is heat-stable, tasteless, and odorless, and is not destroyed by cooking or gastric acid. Symptoms may begin immediately or within several hours of ingestion and may include nausea, vomiting, diarrhea, itching and muscle weakness, aches and spasms. Neurological symptoms may include pain, ataxia (stumbling gait), paresthesias (tingling), and circumoral parasthesias (numbness around the mouth). Sensory reversal of hot and cold sensation when touching or eating objects of extreme temperatures may occur. In severe cases, respiratory failure and cardiovascular collapse may occur. Pruritus (itching) is characteristically made worse by alcohol ingestion. Gastrointestinal symptoms usually disappear within 24 to 72 hours. Although complete recovery will occur in the majority of cases, neurological symptoms may persist for months or years. Signs and symptoms of ciguatera fish poisoning may be misdiagnosed as decompression sickness or contact Dermatitis from unseen fire coral or jellyfish. Because of rapid modern travel and refrigeration, ciguatera poisoning may occur far from endemic areas with international travelers or unsuspecting restaurant patrons.
Prevention
Never eat the liver, viscera, or roe (eggs) of tropical fish. Unusually large fish of a species should be suspected. When traveling, consult natives concerning fish poisoning from local fish, although such information may not always be reliable. A radioimmunoassay has been developed to test fish flesh for the presence of the toxin and soon may be generally available.
First Aid and Treatment
1. Treatment is largely supportive and symptomatic. If the time since suspected ingestion of the fish is brief and the victim is fully conscious, induce vomiting (syrup of Ipecac) and administer purgatives (cathartics, laxatives) to speed the elimination of undigested fish.
2. In addition to the symptoms described above, other complications which may require treatment include hypotension and cardiac dysrhythmias.
3. Antiemetics and antidiarrheal agents may be required if gastrointestinal symptoms are severe. Atropine may be needed to control bradycardia. IV fluids may be needed to control hypotension. Calcium gluconate, diazepam, and methocarbamol can be given for muscle spasm.
4. Amytriptyline has been used successfully to resolve neurological symptoms such as depression.
5. Cool showers may induce itching.

Scombroid Poisoning
Unlike ciguatera poisoning, scombroid fish poisoning occurs from fish that have not been promptly cooled or prepared for immediate consumption. These include tuna, skipjack, mackerel, bonito, dolphin fish, mahi mahi (Pacific dolphin), and bluefish. Fish that cause scombroid poisoning are found in both tropical and temperate waters. A rapid bacterial production of histamine and saurine (a histamine-like compound) produce the symptoms of a histamine reaction: nausea, abdominal pain, vomiting, facial flushing, hives, headache, itching, bronchospasm, and a burning or itching sensation in the mouth. Symptoms may begin one hour after ingestion and last 8 to 12 hours. Death is rare.
Prevention
Immediately clean the fish and preserve by rapid chilling. Do not eat any fish that has been left in the sun or in the heat longer than two hours.
First Aid and Treatment
Oral antihistamine, (e.g., diphenhydramine, cimetidine), epinephrine (given subcutaneously), and steroids are to be given as needed.